
A Cultural Take on Diabetes Self-Management
Filipino Americans are almost twice as likely as White Americans to develop Type 2 diabetes. According to a Healio article, “The prevalence of diabetes was high among Filipino Americans (7.6%) compared with non-Hispanic White Americans (4.3%; P < .01).” On an even broader scale, the rates of Type 2 diabetes diagnoses for non-White American ethnic groups were generally higher than those of White Americans. A study discussed in “Racial and Ethnic Disparities in Prevalence and Care of Patients With Type 2 Diabetes” states that, “The prevalence of diagnosed Type 2 diabetes by racial/ethnic group is as follows: Asians 9.0%, African Americans 13.2%, Hispanic 12.8%, and non-Hispanic Whites 7.6%.”
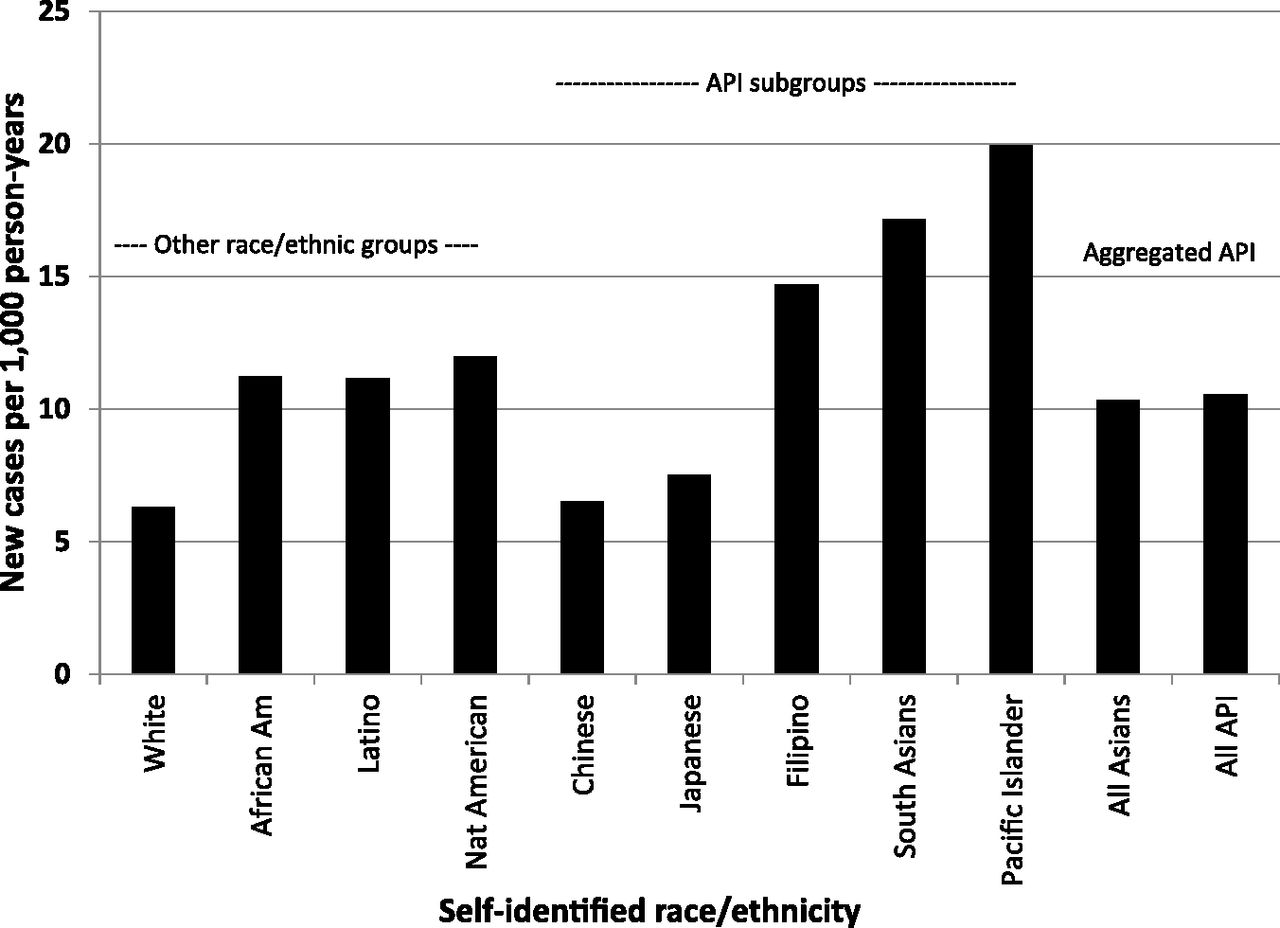
Figure 1. Rates of Diabetes According to Race/Ethnicity (care.diabetesjournals.org)
Disease does not discriminate. “Diabetes is the disease that affects all adults,” said Dr. Marie Agleham. However, health disparities and the critical care gap in American healthcare may contribute to these statistics.
For Type 2 diabetes specifically, lifestyle changes, self-management and programs surrounding those factors are the most common methods of treatment. According to the American Diabetes Association, “Diabetes self-management education and support has been shown to be cost-effective by reducing hospital admissions and readmissions, as well as estimated lifetime health care costs related to a lower risk for complications.” Diabetes self-management education (DSME) programs are effective in lifestyle change treatment and preventative measures for Type 2 diabetes. However, non-White American ethnic groups are still at higher risk despite the same treatment. For Filipino Americans, a study from the American Journal of Manager care states, “The prevalence of diabetes is significantly higher among non-obese Filipino Americans aged 50 and older than in their White counterparts, even after controlling for lifestyle factors.” DSME programs aren’t as effective for other ethnic groups, such as FIlipinos, despite having higher rates of Type 2 diabetes diagnoses.
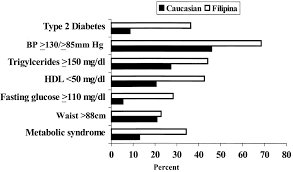
Figure 2. Diabetes statistics of Filipinos and Caucasions.
Dr. Marie Agleham discusses the issue of monolithic treatment, “It’s equality versus equity. They are not the same.”
To address the critical care gap in diabetes self-management treatment, culturally-responsive DSME programs are a proposed solution. The Filipino American Care Experience (FACE) modeled a culturally-responsive DSME program for Filipino-Americans in the Bay Area. Dr. Marie Agleham, one of the FACE physicians who helped organize and teach classes in the program described its structure. Filipino Kaiser patients diagnosed with Type 2 diabetes were invited to attend the class that is held every three months. The classes focused on culturally-specific and healthier recipes. They also encouraged physical activity by incorporating family and other Filipino values.
“They (traditional DSME) do not address foods we eat. Filipinos have a certain diet that makes them at high risk of diabetes. The Filipino family dynamic is a big factor as well. We talk about all of this during our classes while traditional diabetes management classes do not,” said Dr. Agleham, describing why FACE’s culturally-responsive DSME is more successful in prevention and treatment.
Every patient who attends is required to take a follow-up A1C test and their results are recorded. According to Dr. Agleham, participants who attended at least one of their classes and took an A1C test three months following the class showed a decrease in their A1C levels. However, more data isn’t readily available outside this model. A similar discussion-based diabetes management class in Northern California exists for Latino Kaiser patients. FACE is in the progress of expanding and continuing their program to gather more significant data to propose culturally-responsive DSME as an effective solution to one sector of the critical care gap.